Understanding distant recurrence risk from tumor tissue analysis.
After surgery, myStage Dx helps doctors assess distant recurrence risk by analyzing patterns in a routine pathology slide and combining them with standard clinicopathologic information.
Who is myStage Dx designed for?
myStage Dx is designed for adults with a specific type of early breast cancer: node-positive, ER-positive, HER2-negative disease. Your doctor will decide whether it is appropriate based on your diagnosis, treatment history, pathology report, and available tumor tissue.
myStage Dx is not intended for all breast cancers. It is not intended for metastatic disease at diagnosis or cases treated with neoadjuvant chemotherapy.
Your doctor will check two main things.
- Whether your breast cancer type matches the test population.
- Whether a suitable H&E-stained tumor slide is available.
These factors are reviewed by the ordering physician before use.
Why distant recurrence risk matters for your care
For patients with early or localized breast cancer, the cancer has not spread to distant organs. Treatment often starts with surgery and may include radiation therapy or other treatments to reduce recurrence risk.
After surgery, one important question remains: could microscopic cancer cells already be elsewhere in the body and later grow into a distant recurrence, also called metastasis?
Doctors estimate this risk using clinical and pathological variables, such as tumor size, grade, lymph-node involvement and receptor status. In node-positive ER-positive, HER2-negative early breast cancer, these variables can be limited in estimating distant relapse: many patients are considered within the same clinical group, but their true risk of developing metastasis is not the same. Some will relapse, while others will not.
This matters because recurrence risk can inform discussions about treatment intensity. Higher estimated risk may support consideration of additional treatment, while lower estimated risk may support avoiding unnecessary treatment burden.
myStage Dx provides complementary prognostic information related to distant recurrence risk by combining information from a routine pathology slide prepared from tumor tissue with standard clinicopathologic information.
?What is early or localized breast cancer?
Early or localized breast cancer usually means the cancer has not spread to distant organs. Treatment often starts with surgery and may be followed by additional treatment to reduce recurrence risk.
?What is distant recurrence?
Distant recurrence, also called distant relapse or metastasis, means breast cancer returns in another part of the body, such as bone, liver, lung, or brain.
?What information do doctors already use?
Doctors use clinical and pathology information such as tumor size, grade, lymph-node involvement and receptor status. Genomic tests, when used, read selected gene activity in the tumor.
?What is treatment intensity?
Treatment intensity refers to how much treatment is recommended or discussed after surgery. It may include adding treatment or avoiding unnecessary treatment burden, depending on the overall medical context.
Where myStage Dx fits in the care journey.
myStage Dx is typically performed after surgery, when the final pathology report and a suitable slide prepared from tumor tissue are available. The result is intended for physician interpretation with the patient’s clinical and pathology information.
Diagnosis and surgery
Diagnosis and surgery establish the tumor type and remove tissue for pathology review.
Final pathology
The pathology report and a suitable tumor-tissue slide become available after surgery.
myStage Dx analysis
When ordered by a physician, myStage Dx analyzes slide patterns with standard clinicopathologic information.
Physician interpretation
The report provides prognostic information related to distant recurrence risk.
Care discussion
Physicians review results with the overall medical situation and other clinical information.
Different information can show different views of the cancer.
Your care team already uses information such as tumor size, lymph-node involvement, tumor grade, receptor status, overall health and treatment history. myStage Dx provides additional tissue-biology information from prognostic signals decoded from a routine pathology slide prepared from the tumor tissue removed during surgery.
Information doctors already use
Tumor size, lymph-node involvement, tumor grade, ER/PR/HER2 status, overall health, treatment history, and inherited genetic information when relevant.
Biology visible in the tissue slide
myStage Dx analyzes patterns visible in a routine pathology slide prepared from tumor tissue removed during surgery, including tumor architecture, proliferation, and the tumor microenvironment.
Gene activity, when used
Some breast cancer tests measure activity of selected genes in the tumor to help estimate recurrence risk or treatment benefit in specific patient groups.
How a routine tumor slide becomes recurrence-risk information
After surgery, the pathology laboratory prepares a very thin section of tumor tissue and stains it so cells and tissue structures become visible. This is called an H&E slide. H&E slides are routinely reviewed by a pathologist to confirm the diagnosis and assess features that already help doctors understand prognosis.
A single digitized slide can contain millions of cells and a rich representation of tumor biology: how cancer cells are arranged, how often cells appear to be dividing (mitoses), and the surrounding immune and stromal cells that interact with the tumor.
myStage Dx analyzes a digital version of the tumor slide. Using artificial intelligence (AI)-assisted image analysis, it systematically identifies biological elements across the slide and measures tissue patterns at scale, including tumor architecture, proliferation, and microenvironment.
These measurements are used to generate prognostic signals: tissue-based information that helps estimate whether the biology visible on the slide is associated with a higher or lower chance of distant recurrence. Rather than relying on one visible feature alone, the assay captures multiple signals from the tissue image.
The assay was developed using tumor slides and follow-up data from thousands of patients followed over time after cancer diagnosis. This allowed slide patterns to be linked with long-term outcomes, including distant recurrence.
?What is an H&E slide?
H&E stands for hematoxylin and eosin. It is a standard stain used by pathology laboratories to make tumor cells and tissue structures visible under a microscope.
?What is a pathologist?
A pathologist is a physician specialized in diagnosing disease by examining tissue and cells. In breast cancer, the pathologist describes tumor features that help guide care.
?What does AI-assisted analysis do?
It helps identify relevant tissue structures across the digitized slide, measure how these structures are arranged, and turn visual tissue patterns into quantitative information used by myStage Dx.
?What is a prognostic signal?
A prognostic signal is tissue-based information linked to how a cancer may behave over time. myStage Dx uses multiple signals from the tissue image to assess distant recurrence risk.
?Why does follow-up data matter?
Follow-up data show what happened to patients over time after diagnosis and treatment. In the development data set, long-term follow-up helped link slide patterns with later distant recurrence.
What your doctor receives.
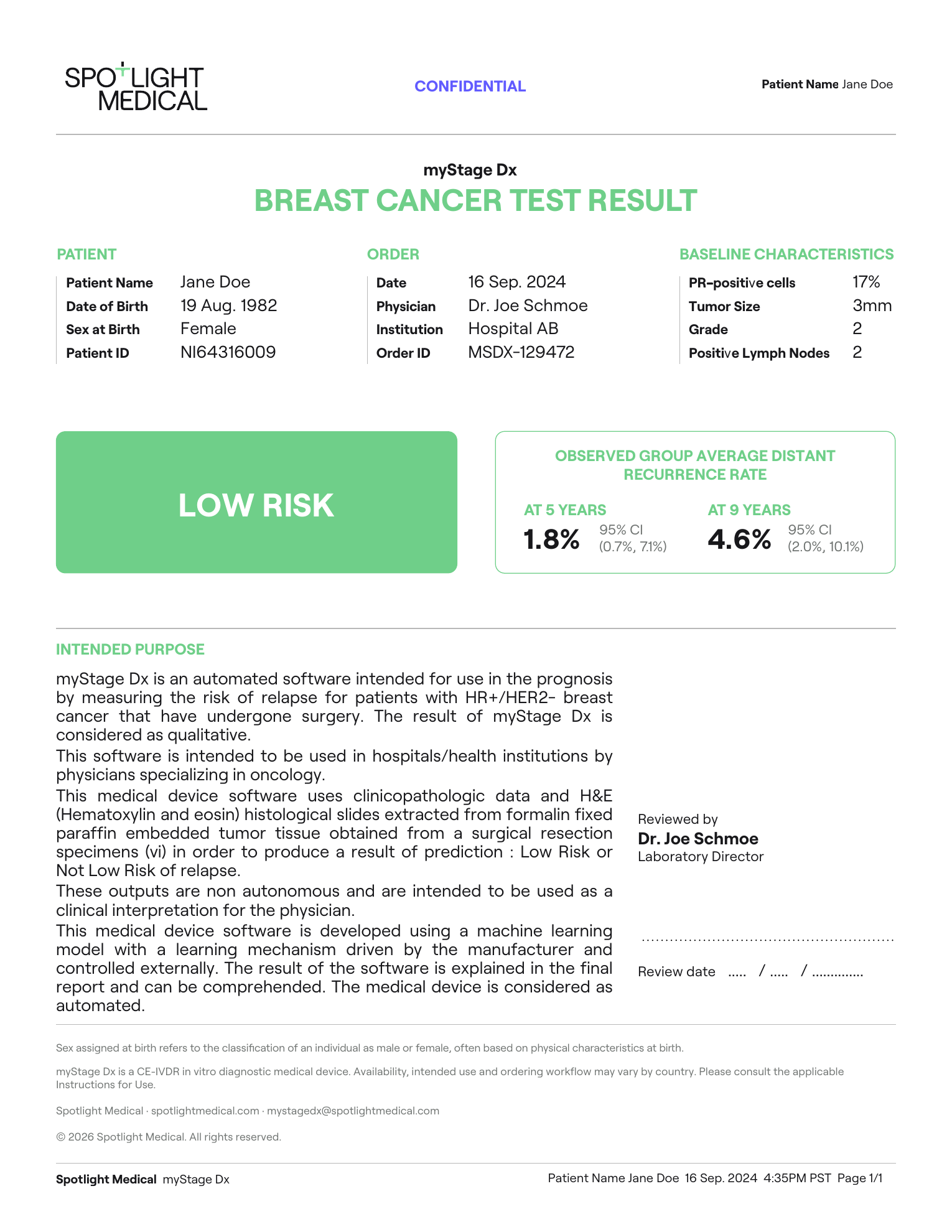
The myStage Dx report is written for the ordering physician. The sample below shows the type of information included in a physician report, such as the result category, information used for analysis, and validation context. It is not intended for patient self-interpretation.
 1
2
3
4
5
1
2
3
4
5
Result category
Shows the myStage Dx classification reported to the ordering physician.
Validation context
Shows group-level validation information included for physician interpretation.
Patient information
Shows sample patient identifiers included in the report.
Order information
Shows sample order details such as ordering physician, institution, and order identifier.
Information used for analysis
Lists the pathology and clinicopathologic information used in the analysis.
This sample is provided for educational purposes. Report interpretation is performed by qualified healthcare professionals in the context of the patient’s medical situation.
What the myStage Dx result means.
The report gives one of two result groups: Low Risk or Not Low Risk. These groups are based on tissue-biology patterns seen in the tumor slide and how those patterns were linked to distant recurrence in clinical validation studies.
A lower distant recurrence risk group
The tumor slide showed patterns associated with a lower observed rate of distant recurrence in validation studies.
A higher distant recurrence risk group
The tumor slide showed patterns associated with a higher observed rate of distant recurrence in validation studies.
Where these numbers come from
These numbers come from clinical validation studies using tumor samples and follow-up information from patients with early breast cancer. In these studies, myStage Dx was applied to patients’ tumor slides and pathology information, and the result groups were compared with what happened to patients over time. The CANTO and UNIRAD cohorts followed patients after diagnosis and treatment, allowing researchers to study distant recurrence over several years. These numbers describe groups of patients, not a guaranteed outcome for one person.
Scientific reference: Bidard F-C, Gessain G, Bachelot T, Frechin L, Vincent-Salomon A, Drubay D, et al. Journal of Clinical Oncology. 2025;43:3090-3101. doi:10.1200/JCO-25-00742.
Plain-language answers.
These answers are general. Your oncology team is the right source for medical advice about your case.
Is myStage Dx for all breast cancers?
No. myStage Dx is designed for adults with stage II-III, node-positive, ER-positive, HER2-negative early breast cancer. The ordering physician determines whether the test fits the diagnosis, treatment history, and available tumor tissue.
Can the test be discussed before surgery?
Yes. The test can be discussed before surgery, but it is typically performed after surgery, once the tumor slide and final pathology information are available.
When would myStage Dx fit into my care?
myStage Dx is usually considered after surgery, when the final pathology report and a suitable tumor slide are available. The result can then provide information for physician interpretation after surgery.
Will I need another biopsy or another surgery?
Usually no. The test is designed to use tumor tissue already available from surgery and routine pathology. Your care team can confirm whether a suitable H&E-stained slide is available.
What if my hospital cannot digitize slides?
A slide-shipment route may be used where available. A representative H&E-stained tumor slide is placed in a collection kit and sent to a designated partner digitization facility before analysis.
Is myStage Dx a genomic test?
No. Gene-activity tests read selected gene activity in the tumor. myStage Dx analyzes tissue patterns visible in a digitized H&E slide, including tumor architecture, proliferation, and the tumor microenvironment.
What do Low Risk and Not Low Risk mean?
They are result groups based on tissue-biology patterns seen in the tumor slide. In clinical validation studies, about 5 in 100 patients in the Low Risk group and about 23 in 100 patients in the Not Low Risk group had distant recurrence by 9 years.
Does Low Risk mean no risk?
No. Low Risk means the result belongs to the lower distant recurrence group defined by the test. It does not mean distant recurrence cannot happen.
Does Not Low Risk mean recurrence is certain?
No. Not Low Risk means the result belongs to a higher distant recurrence group than the Low Risk group. It does not mean recurrence is certain.
Can this test decide my treatment?
No. myStage Dx provides prognostic information. Your doctor interprets the result with your pathology report, clinical information, treatment options, other tests when relevant, and your preferences.
How fast is the report available?
Once all required inputs are received, the report is typically returned to the ordering physician within 1–2 business days. Total time from the doctor’s order may be longer if slide selection, shipping, or digitization is needed first.
Who receives the report?
The ordering physician receives the report. Your doctor or care team should explain the result and what it means in the context of your medical situation.