A clearer prognostic view for early breast cancer.
myStage Dx combines information from a routine H&E slide with standard clinicopathologic variables to assess distant metastasis risk within nine years in adult patients with node-positive, ER-positive, HER2-negative early-stage breast cancer.
* Bidard F-C, et al. Journal of Clinical Oncology. doi:10.1200/JCO-25-00742.
Node-positive ER+/HER2- early breast cancer is not one biology.
Clinical and pathological criteria remain essential, but they do not
always capture the full biological heterogeneity of early breast cancer.
myStage Dx is intended to assess distant-metastasis risk for physician interpretation with standard clinicopathologic information.
Stage, nodal status, grade, tumor size, receptor status and other clinicopathologic factors define the clinical context.
Analysis of routine H&E morphology is combined with key clinicopathologic variables to provide complementary prognostic information for physician interpretation.
Low Risk classification showed about five-fold lower 9-year distant recurrence risk.
In the combined node-positive ER+/HER2- early-stage breast cancer validation cohorts from CANTO (NCT01993498) and UNIRAD (NCT01805271), 123 of 633 patients were classified Low Risk. At nine years, the observed distant recurrence / breast cancer death rate was 4.6% in the Low Risk group and 23.0% in the Not Low Risk group.
Peer-reviewed validations
The peer-reviewed validation study was published in the Journal of Clinical Oncology*. The assay was developed in an ER+/HER2- early breast cancer data set and validated using archived specimens from two prospective cohorts.
Observed distant recurrence / breast cancer death rate after surgery
Observed group-average rates in the combined validation cohorts.
At 5 years
At 9 years
Observed distant recurrence over time
Cumulative incidence of distant recurrence / breast cancer death, by myStage Dx result. The grey line shows the overall cohort for visual context.
Bidard F-C, Gessain G, Bachelot T, Frechin L, Vincent-Salomon A, Drubay D, et al. Identifying patients with low relapse rate despite high-risk estrogen receptor-positive/human epidermal growth factor receptor 2-negative early breast cancer: development and validation of a clinicopathologic assay. Journal of Clinical Oncology. 2025;43:3090-3101. doi:10.1200/JCO-25-00742.
How myStage Dx generates its classification.
myStage Dx combines predefined histological features from a digitized H&E slide with standard clinicopathologic variables for physician interpretation. Methodological details are available in the peer-reviewed Journal of Clinical Oncology publication.
Tissue annotation
myStage Dx automatically annotates relevant structures in the digitized H&E slide, including tumor regions and mitotic figures, to support downstream quantification.
Feature extraction
myStage Dx extracts ten predefined histological features related to tumor architecture, tumor microenvironment and proliferation.
Prognostic model
A predefined Cox proportional hazards model combines these features with clinicopathologic variables to generate the Low Risk or Not Low Risk classification.
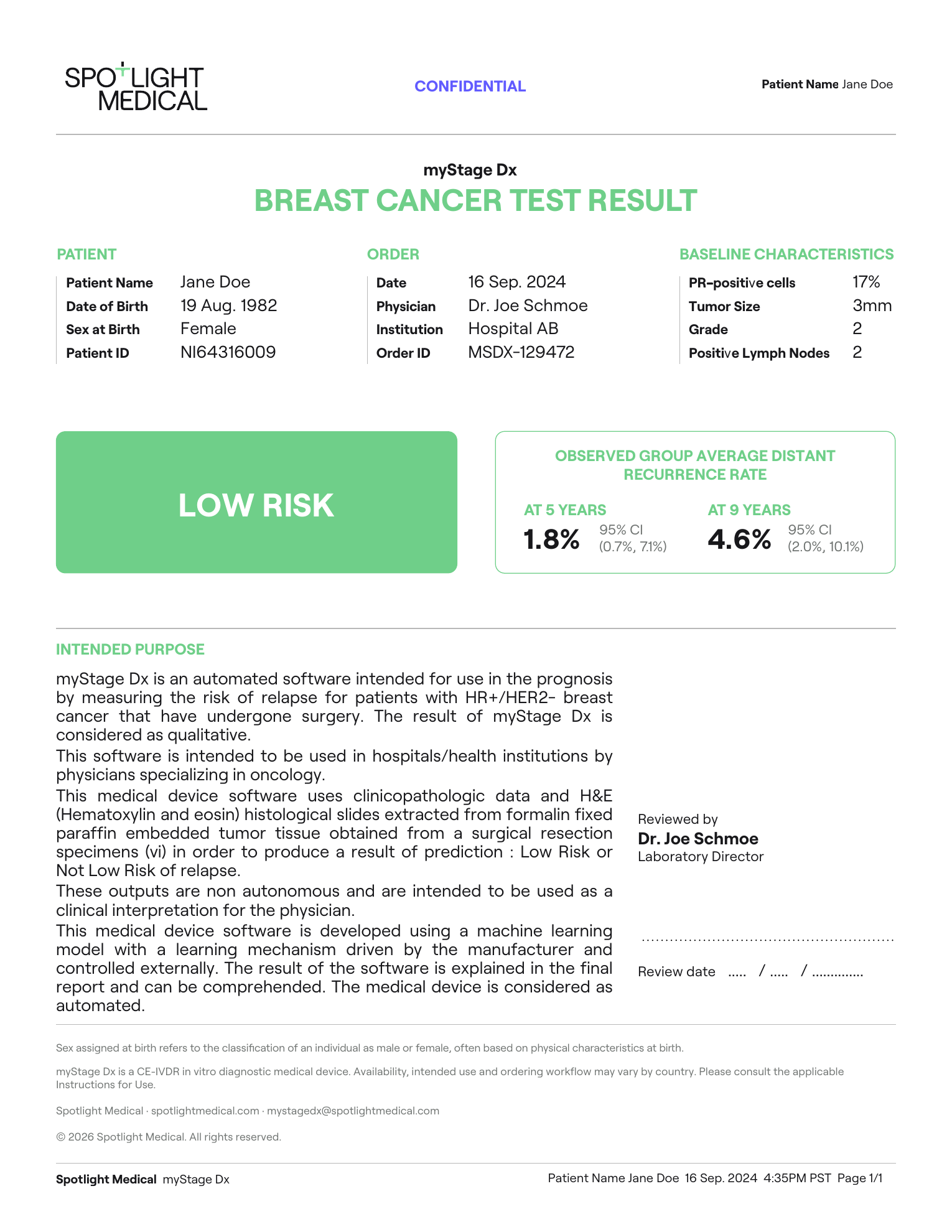
A concise report built for clinical interpretation.
The myStage Dx report presents the prognostic classification, the clinical-pathology inputs used for analysis, and group-level validation context at 5 and 9 years.
 1
2
3
4
5
1
2
3
4
5
myStage Dx result
Displays the binary prognostic classification: Low Risk or Not Low Risk.
Group-level validation context
Shows observed group-average distant recurrence / breast cancer death rates at 5 and 9 years.
Patient section
Contains patient identifiers and demographic fields used for report traceability.
Order information
Documents order date, ordering physician, institution, and order identifier for the report.
Submitted input data
Lists the clinical-pathology inputs used with the H&E slide for analysis.
One workflow, two slide digitization routes.
Ordering is managed through the Spotlight Platform. After site onboarding, the ordering clinician or delegate submits the test request and required clinical-pathology data. Sites with digital pathology infrastructure can upload a validated whole-slide image; sites without local digitization can use the physical slide-shipment pathway.
Set up Spotlight Platform access
New ordering sites contact Spotlight Medical to initiate onboarding. Our team sets up site access in the Spotlight Platform, confirms the ordering clinician and/or ordering delegate, sends login instructions, and reviews specimen logistics, report delivery and support contacts before first use.
Submit the order in the Spotlight Platform
The ordering clinician or delegate confirms patient eligibility and submits the test request with clinical-pathology data for an eligible patient.
Upload digitized H&E WSI
Upload one representative digitized H&E whole-slide image generated through a validated scanner workflow.
Ship one stained H&E slide
Spotlight Medical provides a collection kit. The pathology team places one representative H&E-stained slide in the kit; the slide is shipped to a designated partner digitization facility.
myStage Dx analysis
Once the digitized slide and complete clinical-pathology inputs are received, myStage Dx analyzes the image and variables to generate the binary prognostic classification.
Report returned
The ordering physician receives the myStage Dx report, typically within 1–2 business days after all required inputs are received.
Support for site onboarding and access-pathway review.
myStage Dx access pathways may vary by country and ordering institution. Spotlight Medical supports sites with onboarding, ordering setup, specimen logistics, product documentation and clinical evidence materials needed for institutional or payer review.
Site onboarding and ordering setup
Our team supports Spotlight Platform access, ordering-delegate setup, report-routing configuration and confirmation of the appropriate specimen pathway for your institution.
Coverage and payment support
Where applicable, Spotlight Medical can support benefits investigation, prior authorization documentation, claims-support materials, and payer or institutional review. Final coverage and payment responsibility depend on the patient’s plan, payer policy, country, and ordering pathway.
Questions for oncology, pathology and ordering teams.
Who is myStage Dx intended for?
myStage Dx is intended for adult patients with node-positive, ER-positive, HER2-negative early breast cancer.
What sample is required?
One representative H&E-stained FFPE slide from the primary breast cancer. Sites with validated digital pathology workflows may upload a digitized whole-slide image; sites without local digitization may use the slide-shipment pathway where available.
What if my site cannot digitize slides?
Spotlight Medical can provide a collection kit. The pathology team places one representative H&E-stained slide in the kit, and the slide is shipped to a designated partner digitization facility before software analysis.
Which clinical-pathology data are required?
Nottingham histological grade, pathological invasive tumor size, number of pathologically confirmed positive axillary lymph nodes, and percentage of tumor cells positive for progesterone receptor.
What does the report include?
The report includes the myStage Dx binary prognostic classification, the submitted clinical-pathology inputs used for analysis, and group-level validation context at 5 and 9 years.
How should the result be interpreted?
The result is a prognostic classification. Low Risk identifies patients whose profile was associated with lower observed distant recurrence / breast cancer death rates in validation cohorts. Not Low Risk means the patient did not meet the predefined Low Risk threshold; it does not mean recurrence is certain.
Is myStage Dx a genomic test?
No. myStage Dx is based on a routine H&E whole-slide image combined with clinical-pathology inputs. It does not require RNA expression profiling or genomic sequencing.
Who interprets the result?
myStage Dx is intended for use by physicians specialized in oncology. The result should be interpreted alongside standard clinical, pathological and patient-specific information.
How quickly are results available?
Results are typically available within 1-2 business days once the required digitized slide and complete clinical-pathology inputs have been received.
When should myStage Dx not be used?
myStage Dx is not intended for HER2-positive tumors, hormone receptor-negative tumors, stage IV disease at diagnosis, or cases treated with neoadjuvant chemotherapy, because treatment-induced pathological changes may confound tissue-based analysis. The test also requires sufficient usable FFPE tumor tissue for analysis.
Is myStage Dx certified in the EU?
Yes. myStage Dx is CE-marked under the In Vitro Diagnostic Medical Devices Regulation (IVDR) for its intended use in the European Union. Information about personal data processing is provided in the Privacy Notice.
How are access and reimbursement handled?
Where applicable, Spotlight Medical can support benefits investigation, prior authorization documentation, claims-support materials, and payer or institutional review. Final coverage and payment responsibility depend on the patient’s plan, payer policy, country, and ordering pathway.
Bring myStage Dx into your breast cancer workflow.
Request implementation information, specimen requirements, sample report review, and ordering-pathway details for your site.
- Site onboarding and Spotlight portal setup.
- WSI upload or physical slide-shipment logistics.
- Reimbursement-support documentation and access questions.
Contact: mystagedx@spotlightmedical.com
Contact the myStage Dx team
Share your site details and our team will follow up with relevant implementation and access information.